


COVID Shot-Cancer Links – Understand Them To Defeat Them
Let's explore each of the ways that the COVID vaccines cause cancer and strategies for fighting back

PART 1: Statement of the problem
PART 2: Mechanisms by which the COVID vaccines induce cancer and natural therapies that reverse these
PART 3: Ivermectin’s roles against COVID vaccine-induced cancer
---
PART 1: Statement of the problem
By October 2022, mainstream media could no longer ignore the enormous rise in fourteen different types of cancers in 44 countries around the world and most remarkably in young people. [1] [2] [3] The American Cancer Society acknowledged that cancer mortality has doubled in young people from pre-2020 levels. [4] Pfizer’s 2022 safety report on the COVID-vaccines revealed thousands of cancers of hundreds of types following the injections. [5] By June 2022, there were 3,711 cases reported by Pfizer under that heading.
Oncologists note stark difference in cancers from pre-2020 to the present
UK clinical oncologist Angus Dalgleish, one of the leading oncology researchers in the United Kingdom, sees an alarming number of cancer patients, long in remission, who “ . . . subsequently present with very aggressive relapse when they should have stayed in remission. Sadly, I have yet to find a case where the patients have not received a covid booster vaccine from their GP or hospital because they are ‘at risk.’” [6] His comment on cancer mortality developments around the world is that “the COVID vaccines are linked to cancer and death.” [7]
Canadian oncologist William Makis MD, who has diagnosed over 20,000 cancer patients over his career, says, “I’ve never seen anything like this. . . . I’ve never seen stage four breast cancers presenting in women in their twenties. I’ve never seen stage four colon cancers presenting in men and women in their twenties and thirties . . .These cancers would always present at stage four, and they would always kill them in a matter of a few months, and it was always less than a year. . . ‘Turbo cancer’ is a term that people came up with to describe the extremely aggressive nature of these cancers in the COVID vaccinated, and these cancers behave extremely differently, unlike anything I’ve seen before in my career. . . . And the other feature of these cancers is that they are very resistant to conventional treatment; they’re resistant to radiation therapy, they’re resistant to chemotherapy, and patients seem to be doing very poorly with conventional treatments. Oncologists are really baffled, and they don’t know what to do.“ [8]
Pathologist Ryan Cole MD, formerly of Mayo Clinic, specializes in postmortem examination. He has criticized COVID vaccines for, among other dangers, the severe impairment of the immune system and impairment of the ability to fight cancer. He says “People ask, ‘Do these shots cause cancer? Well, they cause immune suppression. They cause a disruption and a dyregulation of your immune system that is normally what would fight cancer. So that’s what we’re up against. . . . As I travel the world and talk to doctors . . . they are seeing cancers in age groups they have never seen before, and it happened after the rollout of the CV19 shots . . . In 2021, there was about a 6% or 7% increase in cancer. In 2022, there was a 35% increase above average in cancer. . . . People who have been clear of their cancer, 2, 3, 5, 10 and even 20 years, where, after the shots, their cancer aggressively came back, and the estimates are of 17 million people who have died of these mRNA injections. . . . This is a silent holocaust, and that’s what’s sad about this. People were coerced into an experiment, and the deaths are being denied by the medical establishment. . .” [9]
Spike protein dosing from Pfizer and Moderna
The amount of mRNA dose in each Pfizer vaccine is 13 trillion mRNA molecules, and in Moderna is 40 trillion molecules, each enveloped in its own cationic lipid nanoparticle. These figures were determined by molecular weight of each of the two vaccines. [10] To put those numbers in perspective, there are about 30 trillion cells in the human body. So one can imagine the impact of a maximally ubiquitous distribution throughout the whole body, in a roughly one-to-one or one-to-three ratio of payload unit to human cell.
Each of those two vaccines encoded whole spike proteins, and each of the trillions of lipid nano-particle (LNP) enveloped mRNA codes for spike protein. [11]
The Pfizer vaccine was not studied for carcinogenicity or genotoxicity (DNA damage potential) by Pfizer prior to rollout, as we can see from Pfizer’s own documentation to the FDA: [12]
From very early on in the COVID vaccine heyday, February 2021, there was already evidence that COVID vaccines produced a vastly higher spike protein burden in the vaccinated individual than after natural infection. Even within three weeks post-vaccination, the antibodies to spike proteins measured up to 100 times higher in the COVID-vaccinated than in the unvaccinated and previously COVID-infected. [13] While some may interpret these antibodies as a sign of a more intense immune response to spike protein, it also indicates a larger and / or more impactful presence in the body of this known toxin.
Therefore, it is important to fully appreciate the spike protein burden in the vaccinated, in order to be able to find the best strategies to reverse the risk and the damage of this toxin. Toward this end, this article explores the mechanisms of cancer risk from the spike protein. The better we understand these processes, the better we will be able to defend patients and the public against the imminent coming years of record-breaking cancer rates.
It should be noted that the spike protein rarely appears intact more than 20 days after COVID virus infection, but the recombinant, that is, vaccine-generated, spike protein has been observed in the COVID vaccinated, from 69 to 187 days following vaccination. [14] That particular study stopped at 187 days, rather than being the point at which no more spike protein was observed, which implies that there may be a longer time period of spike presence in the bodies of vaccianted people. This persistence includes both the injected mRNA enveloped in liposomes as well as its derivative spike protein. [15] This is plenty of time for the initiation of cancer promoting pathways, and the inhibition of immune defenses against cancer to begin. And it is certainly enough time for cardiovascular and heart damage to have begun, as well as breach of the blood brain barrier, as I discuss in other papers. Peak uptake throughout the northern hemisphere was in spring of 2021. So that is quite a long time for spike protein to persist in the bodies of vaccinated individuals, whereas the fragile mRNA that initiated such spike protein production degrades in weeks, after the payload has been delivered.
Epidemiology of cancer risk following the COVID vaccines
COVID vaccines are correlated with increased incidence of the following cancers.
Lymphomas are so closely correlated with mRNA injection that 45.7% of the studied lymphoma patients who were COVID-vaccinated developed lymphoma within only 30 days post-injection, rather than later. [16] It is not surprising that this is one of the main cancers seen post-COVID vaccine, because the T and B cells of the lymphatic system are not only quickly reproducing, but as waste-drainers, lymph nodes are among the earliest of the body’s tissues to take up spike proteins.
Glioblastomas are pernicious cancers due to their easy accessibility to surrounding brain tissue, and their shielding from most potential treatments behind the blood brain barrier, among other challenges. Pfizer reported hundreds of brain cancers and pre-cancerous conditions in their June 2022 update. [17] Reduced Cytochrome C levels were found in glioma patients post-COVID vaccine, which seemed to be due to impaired oxidative phosphorylation and consequent lower ATP in the mitochondria. [18]
Ovarian and breast cancers are also seen with increased incidence since COVID vaccine rollout, probably due to their p53 impact, yet the COVID vaccines have damaged this p53 gene, the “guardian of the genome” protector of DNA, which I discuss below.
Colorectal cancers have proliferated, and aggressively and among unprecedented young ages since the COVID vaccines. William Dahut is the chief scientif officer of the American Cancer Society. He says, “Colorectal cancer are also presenting with more aggressive disease and larger tumors at diagnosis; it’s more difficult to treat.” Regarding this steep increase in colorectal cancer in youth, Harvard medical professor Kimmie Ng comments that “the steepest rises are in the very youngest people, those in their 20’s and 30’s.” [19]
Although the above are some of the most prominently increased cancers, there is no type of common cancer that has observed to stay flat in incidence since the rollout of the COVID vaccines. All have been listed in the Pfizer documentation. [20]
The Vaccine Adverse Events Reporting System (VAERS), which is overseen by the US Centers for Disease Control (CDC) and the Food and Drug Administration (FDA), is a national surveillance system regarding adverse vaccine effects, for all vaccines given in the U.S., including the mRNA COVID vaccines. For all of the entries regarding cancers in the year 2021, the researchers found that 96% of all the entries for any of the search terms related to cancer were specific to the COVID vaccines, and only 4% for all the other kinds of vaccines put together. [21]
Worldwide, cancer diagnoses and total excess deaths began to rise following the rollout of COVID vaccines, and then to accelerate following the boosters. The findings are most remarkable in younger ages than are typically affected by cancer. [22]
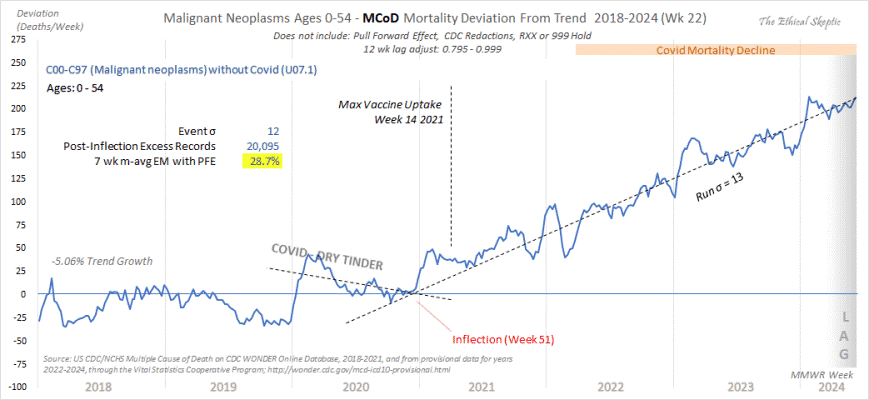
CDC data on cancer mortality summarized below by The Ethical Skeptic shows a sharp inflection point in vastly increased cancer mortality (those with cancer listed as cause of death) in the United States beginning right at the time of the COVID vaccines rollout, the last week of December 2020. In the following graph of cancer mortality in 0 to 54 year olds, the inflection point of when cancer began to increase beyond yearly averages is quite clear, beginning the week after December 14, 2020, when the vaccine first became available. [23] Because this graph shows deviation from trend rather than actual numbers, the curve is often below zero through 2018 – 2020, as cancer mortality was somewhat lower than prior rates then. My other observation is that the first spike after the vaccine rollout likely reflects those who already had fulminant cancer, now worsened by the toxicity of the vaccines, in which case, cancer would have been the default cause of death listed on the death certificate. However, the continuing trend upward of the cancer mortality trend from 2021 to the present is a very strong indicator that a nationwide health-impact event in late 2020-early 2021 caused that sharp increase, and for that we know of only one. All of the following data is derived from CDC reported data.
An enormous study of the entire Japanese population from national vital statistics showed that excess mortality was seen for all cancers examined, 20 types of cancer, each with over 95 or 99% of PI since the rollout of the COVID vaccines. [24] The paper’s politically incorrect findings, based on uncomfortable data, earned its retraction by the journal Cureus. At least 80% of the Japanese population had had two doses of mRNA vaccines and 68% of the population had received a third dose. In that study of the Japanese population, the main cancers to increase following the COVID vaccine rollout were ovarian cancer, leukemia, prostate, lip / oral / pharynx and pancreatic cancers. Breast cancers dipped lower at first, and then shifted to excess mortality also, though the last without statistical significance.
Skyrocketing cases of cancer in the UK have been attributed to smoking, [25] although smoking has drastically decreased in the UK in recent decades, as in the rest of the world. Thirteen new cancers are now being attributed to smoking by the mainstream media, which is highly improbable.
Cancer’s attacks on the body are multi-faceted. They are so complex that researchers Valdes and Perea write:
“This staggering intricacy [of cancer’s many effects] calls for caution when advising all people with cancer (or a previous history of cancer) to receive the COVID-19 primary vaccine series plus additional booster doses.” [26]
To this I would add: Are you a member of a species, such as humans, in which cancer was already the first or second cause of death every year before the COVID vaccines? In that case, the vulnerability is sufficient for all humans to be sure to avoid the COVID vaccines, as I will show in detail below.
PART 2: Mechanisms by which the COVID vaccines induce cancer and natural therapies that reverse these
IgG4 is an antibody made in abundance by COVID-vaccinated persons, many times higher than in the unvaccinated. [27] Antibodies such as the IgG type immunoglobulins are easy to test for by a blood lab, and they are easy to understand. When some irritant – either a pathogenic microbe or allergen – enters the body, then we make reactive antibodies as newly generated soldier molecules to fight the intruders. This is the role of the B-cell generated immunoglobulin antibodies. So when researchers discovered the huge disparity between the COVID vaccinated and the unvaccinated in IgG4 counts, people got excited, and journalists wrote of the stark discovery.
IgG4 is thought to be associated with tolerance of invading microbes, and it is thought that this distracts or shifts the focus of immune system surveillance away from the more inflammatory, combative, so to speak IgG1 and IgG3, and thereby away from important battles against invading pathogens or even cancer. And IgG4 is specifically more tolerant of the SARS-CoV-2 spike protein among other proteins and microbes that do not belong in the body, and that this complacent immune reaction to the spike protein can promote infection and replication by SARS-CoV-2 without opposition. [28]
But there is a problem with all those assumptions and all that attention. IgG4 is a downstream effect, and a product of a vanishingly small component of immune system cells, that is a small fraction of the molecules made by B cells, which comprise only 0.005% = five of every 100,000 blood cells.
That is, IgG4 is unlikely to have as much effect on COVID risk, other microbial risk or cancer risk. But it may serve as a convenient marker on blood labs that gives clues of underlying immune system battles of more importance.
Rather, the most important discovery on COVID vaccine induced cancer risk is something completely different, which is the loss of Type I interferon, and the loss of interferon signalling, in the COVID-vaccinated, which is a tragic loss of many downstream immune functions against cancer. The difference in the importance of these two phenomena is that IgG4 is very rare and very far downstream, while Type I interferon is centrally coordinating of the entire immune system, ubiquitous in healthy people, and significantly reduced in the COVID vaccinated. And this is the central immunity injury that the COVID-vaccinated are faced with. Both of these phenomena are concerning to UK clinical oncologist Angus Dalgleish, who was co-discoverer of the CD-4 receptor. While speaking with U.S. Senator Ron Johnson, Dr. Dalgleish shares his concerns regarding the COVID vaccines, with regard to cancer, is that the COVID vaccine boosters suppress the immune system’s T-cell response, and immunoglubulins switched to tolerization, as two mechanisms most concerning to him by which the COVID vaccines induce or worsen cancer. [29] The Pfizer COVID vaccine specifically was found to significantly reduce Type I interferon, also known as interferon alpha. [30] This causes a tremendous downstream effect of multiple pathologies, both infectious disease and malignant cancer.
Type I interferon, the body’s most important cytokine, is not to be underestimated for its effect against cancer, and this is due to an enormous array of anti-cancer effects. Some of those effects are arrest of the cell cycle, apoptosis, or natural cell death, as well as stimulation of our greatest warriors against cancer, namely the natural killer cells and the CD8+ cytotoxic (“killer”) T-cells. So when COVID-vaccinated individuals display sharply reduced Type I interferon, compared with the unvaccinated, this is a staggering level of vulnerability with respect to cancer.
One of those very important functions is G-quadruplex influence over Type I interferon, which in turn affects transcript, replication and genomic stability. The Seneff research team gets deep into the details of these mechanisms, [31] beyond the scope of this paper, and well worth studying as theirs is the most important analysis to date of the enormity of the COVID vaccine assault on overall immune function.
Cancer attacks the body in seven major ways
At the turn of the millenium, Hanahan and Weinberg identified six major “capabilities” of cancer to undergo changes to promote its own growth and immortality. [32] John Boik summarized the seven major categories of attack inflicted by cancer against the body. [33] I discuss those peculiar features of cancer here, and the roles of vitamins D, C and A against most of those routes of attack. [34] Those are damage or destabilization of DNA, and resulting abnormality in gene expression, abnormal cell signaling and other cell-to-cell communication; angiogenesis, which is the formation of new blood vessels to feed a tumor; invasion and metastasis; as well as immune evasion / camouflage.
I will show throughout this paper that the spike protein carries out most of these functions, in promotion of cancer, and to the detriment of the person with a cancer risk or a cancer burden.
Let’s look at DNA damage first.
Spike proteins damage DNA, and that is a major cancer risk
When DNA is damaged, cancer is a risk. [35] Perhaps the most important cancer risk from the COVID vaccines is damage to DNA. The spike protein has been found by Jiang et al to localize to the cell nucleus, where they were found in abundance and to significantly damage DNA and to alter pathways for DNA repair. The cells most abundant in spike proteins showed the most DNA damage, including the DNA in T-cells and B-cells, showing impairment from this damage. [36] The tragic effect of this is that when spike protein hangs around cells long enough, such as with the mRNA perpetually regenerated spike proteins, your cells’ protective mechanisms against cancer would come to a stop. Not surprisingly, given the current political climate, and despite Jiang and Mei’s meticulously reported data, the Viruses journal retracted their paper, and those who retracted it had financial ties to both Moderna and Pfizer. [37] What Jiang and Mei had proven was what pundits denied, but what Pfizer documentation had already proven: that the spike proteins do enter human cells, and cell nuclei, and do affect DNA.
The SARS-CoV-2 spike protein has been found to cause cells to fuse together to form syncytia, which are multi-nucleated, like cancer cells. And this process has been known to cause cancer. [38] This leads to aneuploidy in daughter cells, which is carcinogenic. Aneuploidy is a different number of chromosomes than the normal 46, either excess or deficient. So DNA is damaged in this way as well, on exposure to spike proteins. [39]
The problem is that DNA repair is essential for B and T cell immunity; it is the core of that adaptive immune system’s ability to defend the organism from both cancerous and infectious disease, [40] and DNA repair is essential to achieve the versatility needed by that adaptive immune system to be able to protect the individual from the variety of infectious and cancerous assaults that each of us faces over the course of life. Indeed, these processes are so fundamental to capable immune surveillance that they are necessary for that ubiquitous and even omniscient monitoring ability of the immune system. Both developing and mature B and T cells, as all cells, need to break and then to repair DNA in order to diversify and to be able to achieve the versatility to accomplish this difficult task.[41] [42] But the spike proteins interfere with this highly complex, evolution-trained and essential immune function. All of these sub-cellular activities are highly organized. Spike proteins throw a kind of microscopic shrapnel into that exquisite system. The damage is so great that Pfizer scientists found that COVID-vaccine injected individuals showed lymphocytopenia (lack of T and B cells) measured two weeks after injection of their second dose. [43]
Cell signaling shutdown, with auto-stimulation and immortality
That was a general view of the damage to DNA from spike protein. Here are some of the specific genetic downstream effects from that damage.
Vaccine developers placed higher guanine-cytosine content in the COVID vaccine RNA than is present in either the wild SARS-CoV-2 virus or in human RNA. These tend to stack into dense formations of guanine bases, which form G-quadruplexes (four guanines stacked together). In excess, this has been found to have downstream effects of dysregulating the G4-protein binding system, which among other diseases, has been found to lead to malignant cancers, by dysregulating human RNA. [44] [45]
The spike protein was found to suppress a p53 dependent gene, leading to tumorigenesis. P53 has been named the “guardian of the genome,” because its well-appreciated function is to prevent cells that have mutated or damaged DNA from reproducing. Of all the body’s proteins, p53 is the most effective suppressor of tumors. P53 accomplishes this by influencing a large set of genes that carry out a variety of functions against cancer. [46] The three major functions of p53 is to stop growth, to repair DNA, and to make sure that a cell dies a normal cell death at the end of its life, rather than gain immortality as cancer cells do. [47] Loss of p53 removes these protective effects for the individual against rampant cancer growth, and nearly half of tumors contain mutated p53. [48] Cancer cells that had high amounts of spike proteins had reduced p53 signalling and reduced p53 transcriptional activity, and after this damage, no controls on cancer cell multiplication were observed. [49] In this way, spike proteins removed an important protective feature against cancer, and then the brakes were released, so to speak, on the proliferation of cancer cells.
Of concern in breast cancer is that the spike protein interacts with BRCA, which is a long-recognized tumor suppressor protein. That protein regulates genes that have effects against cancer. [50] Cancers of the breast, uterus, ovaries and prostate are associated with altered BRCA1 activity. BRCA2 mutations are primarily correlated with cancers of the prostate, pancreas as well as melanoma.
Nuclear factor-kappa B (NFκB) is the name of a group of proteins that cause cancer cells to grow and multiply, while lending them immortality, which makes them a threat to surrounding organs. Spike proteins were found to stimulate and to grow lung cancer by using this NFκB pathway. [51]
Angiogenesis
The NFκB proteins discussed in the previous paragraph create another problem that strengthens cancer to the detriment of the individual, and that is that NFκB stimulates angiogenesis, [52] which is the formation of new blood vessels in the vicinity of the tumor; this is thought to be due to the tumor’s fast-paced metabolism demanding sugar and other fuels, as well as the blood vessel super-highways to satisfy all that demand for fuel, so to speak.
Copper is an essential micronutrient, but must be limited, because of its role in angiogenesis, which has been known since the 1960’s. [53] My clinic has long incorporated zinc in our treatments for cancer, and we have tried to limit copper as much as possible to not stimulate angiogenesis, or to act as an obstacle to it. Zinc is a natural rival opponent of copper.
Immune system evasion
Two issues arise with immune system effects of the COVID vaccines. That is, there is a weakening of the immune system, and there is camouflage or evasion of the immune system by the cancer. Tumors have several mechanisms of camouflage or evasion of targeting by the immune system. [54] The problem is that our immune system’s exist to seek and destroy that which is “non-self,” and tumors disguise themselves, in their antigen display and antigen-concealment, as “self.”
COVID vaccination led to a loss of Type I interferon, which is the immune system’s most important non-nutrient biochemical, which initiates a necessary cascade of immune responses in the event of a pathogenic or cancerous attack. As a result, there are downstream disturbances and failures in the regulation of cancer surveillance. [55]
This leads to increased PD-L1 protein expression on cells, which gives cancer a refuge from immune system surveillance, [56] and functions as a distraction to the immune system with regard to cancer. The PD-L1 protein makes it so that cancer is not apprehended by cells of the immune system, due in part to the distraction of spike protein assault, as an invading pathogen that itself must be fought. The PD-L1 protein has been found to be significantly increased in COVID-vaccinated individuals. [57]
However, the other half of the immune system evasion resulting from decreased Type I interferon is this: The immune system, under the influence of Type I interferon, and then major histocompatibility complex (MHC) class 1 antigen displayed on cancer cells, earmarks and targets cancer cells for the immune system to destroy them. [58] But alas, with the loss of type I interferon, there is a consequent loss of MHC antigen presentation by cancer cells, and thus cancer cells escape the immune system undetected.
The direct effects of Type I interferon against cancer include the above functions plus the following: arrest of the cell cycle (checking rampant growth), tendency toward differentiation (which is a benign rather than a malignant development), initiation of apoptosis (normal “on-time” cell death rather than cell immortality), stimulation of natural killer (NK) cells and cancer-killing (CD8+) T-cells activity. [59]
Also, inactivated COVID vaccines have also been correlated with loss of the very important CD8+ T-cells. [60] As Ryan Cole MD describes this problem, the COVID vaccines “put your T-cells to sleep, in a manner that they can’t fight . . . because those T-cells have gone to sleep to a degree that they would normally fight off cancer, and now they’re not there to fight off cancer.” [61] This also appears to be due to loss of Type I interferon.
In my work with cancer patients over the years, it has been an essential part of our work to keep the immune system vigilant to the presence of cancer and reactive against it. This is very difficult to achieve pharmaceutically, because unlike an obviously foreign item such as a virus or pathogenic bacteria, cancer cells appear to be “self,” and are then too often tolerated without opposition by the immune system. So there is not likely to be a synthetic substance that can accomplish that enhancement of immune vigilance. Vaccines, despite their three-century history, have never achieved such a feat.
Vitamin A, on the other hand, has been able to unmask, so to speak, previously hidden cancers from the immune system, and allow those cancer cells and tumors to be targeted for destruction. On the other hand, it has been found that when vitamin A is deficient, colorectal cancer remained camouflaged from the immune system. [62] This likely has been due primarily to vitamin A’s suppression of the procancerous interleukin IL-6. [63]
The topic of IL-6 bears examination because there is evidence that CD-147, which is abundant on the spike protein, promotes TNF-alpha, which is highly carcinogenic, and that in turn strongly promotes IL-6. [64]
Vitamin A has been able to fight cancer on a number of molecular and cellular levels, beyond the scope of this discussion, [65] but its usefulness against IL-6 alone has been worthwhile. For this reason, vitamin A has been an ever-present part of the cancer-treatment protocols at our clinic since 2006, and at far higher doses than are discussed by the FDA. I have often discussed anywhere from 50,000 to 300,000 units per day with patients, depending on the individual and the aspects of their particular cancer. The success of our clinic’s results against cancer are likely due not to any one of the treatments that we use, but to the synergy among well-tolerated and compatible nutrients that have complementary anti-cancer effects.
Metastasis: an invasion of tumors at sites near and far from the primary tumor
When matched with an unexposed control group, the SARS-CoV-2 spike protein was found to stimulate the migration of lung cancer cells through the blood, and subsequent invasion of the basement membrane in a new location in the body. [66] That process is known as metastasis. Not only do cancer cells break off from a primary tumor to then travel in the bloodstream, but weak basement membranes of different bodily organs are fertile ground for a new secondary tumor to gain a foothold. Think of this as for example, an old ceramic coffee cup with a scratched surface in one area. That area is where the coffee will seep into and stain more so than the resilient finish of the rest of the cup. Similarly, the basement membranes that protect our cells are most vulnerable to a new metastasizing cancer cell floating by in the blood at that weak area rather than where the basement membrane is intact and thereby more resilient to such penetration.
My clinic, since 2006, has fought against basement membrane weakness and friability; that is, our clinic has worked to strengthen our cancer patients’ basement membrane resilience against metastatic invasion. Vitamin C is a necessity, not a luxury, for building collagen, which I describe to patients as the equivalent of the bricks and mortar that we are made of, because collagen is by far the most abundant of the proteins in the body. This is never recognized as the reason for vitamin C’s good effect against cancer, but I think it is one of the most important of its mechanisms. There are dozens of types of collagen. Pro-collagen requires vitamin C together with the amino acids lysine and proline. Therefore, we prepare IV nutrient treatments for the cancer patients that include these three ingredients.
Other mechanisms of the COVID vaccines that promote cancer
The above mechanisms of the COVID vaccines against cancer are those with the most available evidence, and historically established as known cancer promoting pathways. However, there is also accumulating evidence of additional cancer causing factors that are new and peculiar to these novel injections.
DNA plasmid contamination of the COVID vaccines
Foreign DNA , which derives from amplification in the bacteria E. coli, contaminates both the Pfizer and Moderna vaccines. This is a different but related problem than the problem of damage to human DNA that I describe above.
Dr. Phillip Buckhaults is a cancer genomics expert. He testifed, in a video that is no longer viewable on YouTube, to the South Carolina Senate on this DNA contamination found in COVID vaccines. He testified: “The Pfizer vaccine is contaminated with DNA. It’s not just mRNA. I’m kind of alarmed about the possible consequences of this. . . . OIt could be causing some of the rare but serious side effects like death from cardiac arrest. This DNA can and likely will integrate into the genomic DNA of cells that got transfected with the vaccine mix. It’s different from RNA because it can be permanent. It could cause theoretically a sustained autoimmune attack toward that tissue. It’s also a very real theoretical risk of future cancer in some people. There’s probably about 200 billion pieces of this plasmid DNA in each dose of the vaccine . . . This is a bad idea.” [67]
Kevin McKernan was the first to discover and to write about this problem of plasmid DNA contamination of the COVID vaccines. [68] This was confirmed by Speicher and Rose. [69]
“Why does that matter?” asks pathologist Ryan Cole. “That matters because that [E coli derived plasmid] DNA can park itself in the nucleus of your cell next to your own DNA, and piggy-back a ride into the next generation of cell, into the next generation of cell, etc. So can it become part of the next generation that’s born? It could. . . And this did happen in mouse studies up to four litters of mice.” [70]
Methyl-pseudouridine
N1-Methyl-pseudouridine (M1Ψ) was inserted into the manufactured mRNA used in the COVID vaccines, which produced a genetically-modified RNA, in order to stabilize the spike protein long enough to display it to the immune system, for recognition as a foreign antigen, so that the immune system could make antibodies against the spike proteins. However, this create new problems, including for cancer risk. It turned out that the M1Ψ actually stimulated both cancer growth and metastasis in melanoma. [71] Nevertheless, N1-methyl pseudouridine is naturally occurring in human RNA, comprising 1.4% of all bases in our RNA, and is necessary for our protein synthesis. [72] So I doubt that this is a major cause of cancer, except by the indirect route of giving shelter from immune attack to spike protein production.
Other possible mechanisms of the increased rates of cancer being seen are an alleged contamination of the COVID vaccines by the oncogenic SV40 virus, the CD147 presence in the spike protein favoring the carcinogenic TNF-alpha,[73] as well as possible contribution to cancerous processes by microclots induced by the spike proteins.
PART 3: Ivermectin’s roles against COVID vaccine-induced cancers
Ivermectin is one of the safest drugs in existence. Prior to the COVID era, four billion doses had been given around the world in the half century since its discovery, mostly in equatorial Africa, as ivermectin has excellent effects against tropical parasites. However, it has been crucially important in the COVID era, because spike protein is the main toxin in both naturally acquired COVID infection as well as in the COVID vaccines. In the latter case, those full-length spike proteins are produced by the mRNA template. I had cited studies back in 2021, in my book The Defeat of COVID, in which several teams of researchers had each shown that ivermectin effectively blocks the troublesome ends of the spike protein, both S1 moieties as well as S2, and that humanity would be fortunate if ivermectin blocked even one of those, let alone the much better effect of blocking all three.
Since that time, many more effects of ivermectin against spike protein have been found. Clinical oncologist William Makis MD summarizes fifteen of those. [74]
Essentially, ivermectin is able to not only block most of the worst effects of the mRNA vaccines, but it inhibits tumor growth and arrests the cell cycle of cancer, and in the very well tolerated dose of 2 mg / kg body weight, which is roughly 136 mg dosing for a 150-lb person or 182 mg for a 200-lb person, and is compatible with both conventional chemotherapy as well as nutritional cancer therapies.
Remarkably, ivermectin was shown to oppose cancer stem cells. [75] Those stem cells are what enable cancer to grow and later to recur. I say that it is remarkable, because previously, only vitamin C had been known to kill cancer stem cells, [76] [77] while being harmless to normal cells. [78]
Even at lower doses, studies summarized in the Makis paper have shown tumor reductions of 50% to 85% in some of the most devastating cancers caused by the COVID vaccines, namely glioblastomas, cancers of the colon and breast. In vitro studies found ivermectin’s effect against a wider range of cancers, including the aforementioned, as well as pancreatic, ovarian, prostate and melanoma.
Regarding pancreatic cancer, ivermectin was found to be compatible with, and to outperform, the standard pancreatic chemotherapy drug gemcitabine, in its effect against that cancer. [79]
--
I look forward to observing more and writing more as time goes on about the life-saving effects of ivermectin and other harmless interventions against not only COVID, but against the most common cancers of our time, especially those that have proliferated since the rollout of the COVID vaccines.
Endnotes
[1] B Goodman. A global epidemic of cancer among people younger than 50 could be emerging. Oct 17 2022. CNN. https://www.cnn.com/2022/10/14/health/early-onset-cancer-increase/index.html
[2] T Ugai, N Sasamoto, et al. Is early-onset cancer an emerging global epidemic? Current evidence and future implications. Oct 2022. Nature. 19. https://www.nature.com/articles/s41571-022-00672-8.epdf
[3] Agence France Presse. Cancer surging among under 50’s worldwide, study says. Sep 6 2023. Barron’s. https://www.barrons.com/news/cancer-surging-among-under-50s-worldwide-study-says-326d064e
[4] P Kory, M Pfeiffer. Princess Catherine is one of many more young adults with cancer. Washington Times. Mar 26 2024. https://www.washingtontimes.com/news/2024/mar/26/princess-catherine-is-one-of-many-more-young-adult/
[5] Pfizer. APPENDIX 2.2: Cumulative and Interval Summary Tabulation of Serious and Non-Serious Adverse Reactions from Post-Marketing Data Sources BNT162B2 Cumulative Reporting Period: Through 18-JUN-2022. https://www.scribd.com/document/695603788/Pfizer-Phase-III-Appendix-2-2-Cumulative-and-Interval-Summary-of-Serious-and-Non-serious-Adverse-Reactions-From-Post-Marketing-Sources-as-at-21-Jun
[6] W Makis. Video – Oncologist Prof. Dalgleish warns about turbo cancer (April 2024). Jul 2 2024. MakisMD.

[7] A Dalgleish. Systematic suppression of the truth – COVID vaccines are linked to cancer and death. Jul 11 2024. Conservative Woman. https://www.conservativewoman.co.uk/systematic-suppression-of-the-truth-covid-vaccines-are-linked-to-cancer-and-death/
[8] J Ferguson. Video: Dr. William Makis on turbo cancer: I’ve never seen cancers behaving like this. Oct 13 2023. https://rumble.com/v3ssk1q-must-watch-dr.-william-makis-on-turbo-cancer-ive-never-seen-cancers-behavin.html
[9] R Cole. CV19 vax causes turbo cancer – Dr. Ryan Cole. Oct 2023. Greg Hunter’s USAWatchdog.com https://rumble.com/v3og3mw-cv19-vax-causes-turbo-cancer-dr.-ryan-cole.html
[10] K McKernan, A Kyriakopoulos, et al. Differences in vaccine and SARS-CoV-2 replication derived mRNA: Implications for cell biology and future disease. Nov 24 2021. OSF Preprints. https://osf.io/preprints/osf/bcsa6
[11] G Poland, I Ovsyannikova, et al. SARS-CoV-2 immunity: review and applications to phase 3 vaccine candidates. Oct 13 2020. Lancet. 396 (10262). 1595-1606. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7553736/
[12] Pfizer Worldwide Safety. 5.3.6 Cumulative analysis of post-authorization adverse event reports of P-07302048 (BNT162B2) received through 28 Feb 2021. P. 59. https://phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf
[13] F Gobbi, D Buonfrate, et al. Antibody response to the BNT162b2 mRNA COVID-19 vaccine in subjects with prior SARS-CoV-2 infection. Feb 28 2021. Viruses. 13 (3). 422. https://www.mdpi.com/1999-4915/13/3/422
[14] C Brogna, S Cristoni, et al. Detection of recombinant spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms. Aug 31 2023. Proteomics Clin Appl. https://onlinelibrary.wiley.com/doi/10.1002/prca.202300048
[15] L Boros, A Kyriakopoulos, et al. Long-lasting, biochemically modified mRNA, and its frameshifted recombinant spike proteins in human tissues and circulation after COVID-19 vaccination. Jun 12 2024. Pharmacol Res Perspect. 12 (3). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11169277/
[16] Z Cui, J Cheng. A systematic review of lymphoma secondary to COVID-19 vaccination. Authorea. Sep 4 2024. https://www.authorea.com/users/827829/articles/1222329-a-systematic-review-of-lymphoma-secondary-to-covid-19-vaccination
[17] Pfizer. APPENDIX 2.2: Cumulative and Interval Summary Tabulation of Serious and Non-Serious Adverse Reactions from Post-Marketing Data Sources BNT162B2 Cumulative Reporting Period: Through 18-JUN-2022. https://www.scribd.com/document/695603788/Pfizer-Phase-III-Appendix-2-2-Cumulative-and-Interval-Summary-of-Serious-and-Non-serious-Adverse-Reactions-From-Post-Marketing-Sources-as-at-21-Jun
[18] H Abramczyk, B Brozek-Pluska, et al. Decoding COVID-19 mRNA vaccine immunometabolism in central nervous system: human brain normal glial and glioma cells by Raman imaging. Mar 2 2022. bioRxiV. https://www.biorxiv.org/content/10.1101/2022.03.02.482639v1
[19] P Kory. We published an op-ed on the unprecedented rise of cancers in young people and questioned the link to mRNA vaccines. Mar 27 2024. Pierre Kory Medical Musings.

[20] Pfizer Worldwide Safety. 5.3.6 Cumulative analysis of post-authorization adverse event reports of P-07302048 (BNT162B2) received through 28 Feb 2021. P. 59. https://phmpt.org/wp-content/uploads/2022/04/reissue_5.3.6-postmarketing-experience.pdf
[21] S Seneff, G Nigh, et al. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes and microRNAs. Jun 2022. Food Chem Toxicol. 164 (113008). https://www.sciencedirect.com/science/article/pii/S027869152200206X
[22] A Powell. Cancer keeps coming for the young. Why? Feb 6 2024. The Harvard Gazette. https://news.harvard.edu/gazette/story/2024/02/cancer-keeps-coming-for-the-young-why/
[23] The Ethical Skeptic. The state of things pandemic, we have a cancer emergency. Week 38, 2024. https://theethicalskeptic.com/2024/10/02/the-state-of-things-pandemic-week-38-2024/
[24] M Gibo, S Kojima, et al. Increased age-adjusted cancer mortality after the third mRNA-lipid nanoparticle vaccine dose during the COVID-19 pandemic in Japan. Apr 8 2024. [Retracted by Cureus]. https://www.cureus.com/articles/196275-increased-age-adjusted-cancer-mortality-after-the-third-mrna-lipid-nanoparticle-vaccine-dose-during-the-covid-19-pandemic-in-japan#!/
[25] M Searles. Rates of cancer caused by smoking hit record highs. Jul 9 2024. The Telegraph. https://www.telegraph.co.uk/news/2024/07/09/rates-of-cancer-caused-by-smoking-hit-record-highs/
[26] R Valdes, Y Perea. SARS-CoV-2 vaccination and the vaccination and the multi-hit hypothesis of oncogenesis. Dec 17 2023. Cureus. https://www.cureus.com/articles/209584-sars-cov-2-vaccination-and-the-multi-hit-hypothesis-of-oncogenesis
[27] P Irrgang, J Gerling. Class switch toward non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. Dec 22 2022. Science. 8 (79). https://www.science.org/doi/10.1126/sciimmunol.ade2798
[28] V Uversky, E Redwan, et al. IgG4 antibodies induced by repeated vaccination may generate immune tolerance to the SARS-CoV-2 spike protein. May 17 2023. Vaccines (Basel). 11 (5). 991. https://pmc.ncbi.nlm.nih.gov/articles/PMC10222767/
[29] A Dalgleish. This strong evidence of the link between covid vaccines and cancer can no longer be ignored. Apr 24 2024. https://www.conservativewoman.co.uk/this-strong-evidence-of-the-link-between-covid-vaccines-and-cancer-can-no-longer-be-ignored/
[30] K Föhse, B Geckin, et al. The impact of BNT162b2 mRNA vaccine on adaptive and innate immune responses. Oct 2023. Clin Immunol. 255 (109762). https://www.sciencedirect.com/science/article/pii/S1521661623005259
[31] S Seneff, G Nigh, et al. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes and microRNAs. Jun 2022. Food Chem Toxicol. 164 (113008). https://www.sciencedirect.com/science/article/pii/S027869152200206X
[32] D Hanahan, R Weinberg. The hallmarks of cancer. Jan 7 2000. Cell. 100 (1). 57-70. https://www.cell.com/cell/fulltext/S0092-8674(00)81683-9
[33] J Boik. Natural Compounds in Cancer Therapy. Book. Oregon Medical Press. 2001. P. 2.
[34] C Huber. Defeating cancer requires more than one treatment method: An 11-year retrospective case series using multiple nutritional and herbal agents, 2017 update. Dec 30 2017. Nature Works Best Clinic. https://natureworksbest.com/wp-content/uploads/2018/01/2017-Cancer-treatment-paper.2017.12.30.pdf
[35] T Gemoli, G Auer, et al. Genetic instability and disease prognostication. 2015. Recent Results Cancer Res. 200. 81-94. https://pmc.ncbi.nlm.nih.gov/articles/PMC7737009/
[36] H Jiang, Y Mei. SARS-CoV-2 spike impairs DNA damage repair and inhibits V(D)J recombination in vitro. Oct 13 2021. [Retracted by Viruses]. 13 (10). 2056. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8538446/
[37] A Syed. Welcome to Gilead. Jul 30 2022.
[38] C Merle, P Lagarde, et al. Acquisition of cancer stem cell capacities after spontaneous cell fusion. Mar 7 2021. BMC Cancer. 21. 241. https://pmc.ncbi.nlm.nih.gov/articles/PMC7938600/
[39] Y Lazebnik. Cell fusion as a link between the SARS-CoV-2 spike protein, COVID-19 complications and vaccine side effects. Dec 7 2021. Oncotarget. 12 (25). 2476-2488. https://pmc.ncbi.nlm.nih.gov/articles/PMC8664391
[40] J Bednarski, B Sleckman. At the intersection of DNA damage and immune responses. Apr 2019. Nat Rev Immunol. 19 (4). 231-242. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6438741/
[41] A Ciccia, S Elledge. The DNA damage response: Making it safe to play with knives. Oct 22 2010. Mol Cell. 40 (2). 179-204. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2988877/
[42] B Helmink, B Sleckman. The response to and repair of RAG-mediated DNA double-stranded breaks. Jan 3 2012. Annu Rev Immunol. 30. 175-202. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4038028/
[43] E Walsh, R Frenck, et al. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. Oct 14 2020. NEJM. 383. 2439-2450. https://www.nejm.org/doi/pdf/10.1056/NEJMoa2027906
[44] A Wolfe, K Singh, et al. RNA G-quadruplexes cause eIF4A-dependent oncogene translation in cancer. Sep 4 2014. Nature. 513 (7516). 65-70. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4492470/
[45] K McKernan, A Kyriakopoulos, et al. Differences in vaccine and SARS-CoV-2 replication derived mRNA: Implications for cell biology and future disease. Nov 24 2021. OSF Preprints. https://osf.io/preprints/osf/bcsa6
[46] E Kastenhuber, S Lowe. Putting p53 in context. Sep 7 2017. Cell. 170 (6). 1062-1078. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5743327/
[47] S Read. Human Molecular Genetics 2. Chapter 18. 1999. Cancer Genetics. Quoted in https://www.bioinformatics.org/p53/introduction.html
[48] S Zhang, L Carlsen, et al. Advanced strategies for therapeutic targeting of wild-type and mutant p53 in cancer. Feb 28 2022. Biomolecules. 12 (4). 548. https://www.mdpi.com/2218-273X/12/4/548
[49] S Zhang, W El-Deiry. SARS-CoV-2 spike S2 subunit inhibits p53 activation of p21 (WAFI), TRAIL death receptor DR5 and MDM2 proteins in cancer cells. Apr 15 2024. BioRxiv. https://www.biorxiv.org/content/10.1101/2024.04.12.589252v1.full
[50] N Singh, A Singh. S2 subunit of SARS-nCoV-2 interacts with tumor suppressor protein p53 and BRCA: an in silico study. Oct 2020. Transl Oncol. 13 (10). https://www.sciencedirect.com/science/article/pii/S1936523320303065
[51] M Kim, J Kim, et al. The SARS-CoV-2 spike protein induces lung cancer migration and invasion in a TLR2-dependent manner. Sep 13 2023. Cancer Comm (Lond). 44 (2). 273-277. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10876188/
[52] S Huang, C Pettaway, et al. Blockade of NF-kappaB activity in human prostate cancer cells is associated with suppression of angiogenesis, invasion and metastasis. Jul 2001. Oncogene. 20 (31). 4188-4197. https://pubmed.ncbi.nlm.nih.gov/11464285/
[53] M Ziche, J Jones, et al. Role of Prostaglandin E-1 and copper in angiogenesis. Aug 1982. J Natl Cancer Inst. 69 (2). 475-482. https://pubmed.ncbi.nlm.nih.gov/6180207/
[54] D Vinay, E Ryan, et al. Immune evasion in cancer: mechanistic basis and therapeutic strategies. Dec 2015. Seminars in Cancer Biol. 35. S185-S198. https://www.sciencedirect.com/science/article/pii/S1044579X1500019X
[55] S Seneff, G Nigh, et al. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes and microRNAs. Jun 2022. 164. https://www.sciencedirect.com/science/article/pii/S027869152200206X
[56] A Dalgleish. This strong evidence of the link between covid vaccines and cancer can no longer be ignored. Apr 24 2024. https://www.conservativewoman.co.uk/this-strong-evidence-of-the-link-between-covid-vaccines-and-cancer-can-no-longer-be-ignored/
[57] L Loacker, J Kimpel, et al. Increased PD-L1 surface expression on peripheral blood granulocytes and monocytes after vaccination with SARS-CoV-2 mRNA or vector vaccine. Oct 18 2022. Clin Chem and Lab Med. 61 (1). https://www.degruyter.com/document/doi/10.1515/cclm-2022-0787/html
[58] R Heise, P Amann, et al. Interferon alpha signalling and its relevance for the upregulatory effect of transporter proteins associated with antigen processing (TAP) in patients with malignant melanoma. Jan 6 2016. PLoS One. 11 (1). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4703378/
[59] W Schneider, M Chevillotte, et al. Interferon-stimulated genes: A complex web of host defenses. Feb 6 2014. Annu Rev Immunol. 32. 513-545. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4313732/
[60] J Liu, J Wang, et al. Comprehensive investigations revealed consistent pathophysiological alterations after vaccination with COVID-19 vaccines. Oct 26 2021. Nature. 7 (99). https://www.nature.com/articles/s41421-021-00329-3.pdf
[61] R Cole. CV19 vax causes turbo cancer – Dr. Ryan Cole. Oct 2023. Greg Hunter’s USAWatchdog.com https://rumble.com/v3og3mw-cv19-vax-causes-turbo-cancer-dr.-ryan-cole.html
[62] P Huynh, E Beswick, et al. Impaired vitamin A metabolism in colorectal cancer stromal cells: Role in tumor immune evasion. May 2013. Gastroenterology. 338. S-71. https://www.gastrojournal.org/article/S0016-5085(13)60262-0/pdf
[63] R Villéger, M Chulkina, et al. Disruption of retinol-mediated IL-6 expression in colon cancer-associated fibroblasts: new perspectives on the role of vitamin A metabolism. Apr 26 2023. Oncotarget. 14. 377-381. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10132993/
[64] P Chambers. The CD147 epitope on SARS-CoV-2 and the spike in cancer, autoimmunity and organ fibrosis. Nov 3 2023. Qeios. https://www.qeios.com/read/S86J75
[65] C Applegate, M Lane. Role of retinoids in the prevention and treatment of colorectal cancer. Oct 15 2015. World J Gastrointest Oncol. 7 (10). 184-203. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4606174/
[66] M Kim, J Kim, et al. The SARS-CoV-2 spike protein induces lung cancer migration and invasion in a TLR2-dependent manner. Sep 13 2023. Cancer Comm (Lond). 44 (2). 273-277. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10876188/
[67] P Buckhaults. Testimony before the South Carolina Senate. Sep 14 2023.
[68] K McKernan, Y Helbert, et al. Sequencing of bivalent Moderna and Pfizer mRNA vaccines reveals nanogram to microgram quantities of expression vector dsDNA per dose. Open PDF from: https://files.osf.io/v1/resources/b9t7m/providers/osfstorage/64348a3848245638fab48a50?action=download&direct&version=5
[69] D Speicher, J Rose, et al. DNA fragments detected in monovalent and bivalent Pfizer BioNTeach and Moderna modRNA COVID-19 vaccines from Ontario, Canada: Exploratory dose response relationship with serious adverse events. Oct 19 2023. OSF Preprints. https://osf.io/preprints/osf/mjc97
[70] R Cole. CV19 vax causes turbo cancer – Dr. Ryan Cole. Oct 2023. Greg Hunter’s USAWatchdog.com https://rumble.com/v3og3mw-cv19-vax-causes-turbo-cancer-dr.-ryan-cole.html
[71] A Rubio-Casillas, D Cowley, et al. Review: N1-methyl pseudouridine (M1 Ψ): Friend or foe of cancer. May 2024. Intl J Biol Macromolecules. 267 (1). https://www.sciencedirect.com/science/article/abs/pii/S0141813024022323
[72] M Penzo, L Montanaro. Turning uridines around: Role of RNA pseudouridylation in ribosome biogenesis and ribosomal function. Jun 5 2018. Biomolecules. 8 (2). 38. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6023024/
[73] P Chambers. The CD147 epitope on SARS-CoV-2 and the spike in cancer, autoimmunity and organ fibrosis. Nov 3 2023. Qeios. https://www.qeios.com/read/S86J75
[74] W Makis. Ivermectin and cancer: it has at least 15 anti-cancer mechanisms of action. Can ivermectin treat COVID-19 mRNA vaccine-induced turbo cancers? 9 ivermectin papers reviewed. Oct 2 2023.
[75] A Samy, M Hussein, et al. Eprinomectin: a derivative of ivermectin suppresses growth and metastatic phenotypes of prostate cancer cells by targeting the beta-catenin signaling pathway. May 12 2023. J Cancer Res Clin Onc. 149. 9085-9104. https://link.springer.com/article/10.1007/s00432-023-04829-5
[76] L Hongwei, C Wang, et al. Vitamin C preferentially kills cancer stem cells in hepatocellular carcinoma via SVCT-2. Jan 8 2018. Nature. https://www.nature.com/articles/s41698-017-0044-8
[77] Y Seyama, K Sudo, et al. Ascorbic acid predominantly kills cancer stem cell-like cells in the hepatocellular carcinoma cell line Li-7 and is more effective at low cell density and in small speroids. May 21 2024. 709. https://www.sciencedirect.com/science/article/pii/S0006291X24003528
[78] Q Chen, M Espey, et al. Pharmacologic ascorbic acid concentrations selectively kill cancer cells; Action as a pro-drug to deliver hydrogen peroxide to tissues. Sep 12 2005. 102 (38). https://pmc.ncbi.nlm.nih.gov/articles/PMC1224653/
[79] D Lee, H Kang, et al. Ivermectin and gemcitabine combination treatment induces apoptosis of pancreatic cancer cells via mitochondrial dysfunction. Aug 25 2022 Frontiers Pharmacol. 13-2022. https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2022.934746/full